By Hanna Szukalska (tekst dostępny również w języku polskim)
Underfunded, overstretched, short-staffed, over-medicalised, and still mostly based on psychiatric hospitals – for years, the mental health care system in Poland has been in a permanent state of crisis.
“I was diagnosed as schizophrenic myself – wrongly, as it turned out – and hospitalised several times. I know what it means to be stuffed with antipsychotics and strapped down. The label of a mental illness and standard treatment took ten years of my life away,” says Mateusz Biernat, a mental crisis consultant at the Pedagogical University in Kraków, therapist, and member of the Ministry of Health’s mental health advisory board.
“The dominant way of thinking about people with mental disorders in Poland is as a threat that is to be isolated. In this regard, mental health care has hardly changed in 100 years – the most difficult cases are isolated,” says Biernat.
“Sometimes a life-changing diagnosis of a disorder is given after one brief meeting with a psychiatrist – and then you live with it for years,” he adds, visibly frustrated. “But a person is much more than a set of signs and symptoms – first you need to listen and find out more about their experiences and the environment they live in before making a diagnosis of a mental disorder.”
This is confirmed by a report showing that in 2012 almost 15,000 first-time psychiatric consultations resulted in a diagnosis of schizophrenia.
A diagnosed mental disorder in Poland means stigmatisation – not only from society and potential employers. People classed as “mentally ill” are unable to marry without a court order. Spending time in hospital, and being labelled as “crazy”, makes it extremely hard to go back to functioning as part of society.
How the system works
Contact with the Polish mental health care system can begin in various ways: from a visit to a mental health clinic to being admitted to a psychiatric hospital. The latter path is faster, but reserved for people in situations endangering their lives or health, such as strong suicidal thoughts or psychosis.
In less dramatic cases, after contacting a clinic, patients get an appointment to see a psychiatrist, with waiting times up to several months. When they do manage to see someone, the doctor decides on the next step – referring them for psychotherapy or to a suitable institution, such as a stay in a psychiatric hospital for diagnosis, to an open ward or a rehabilitation centre. Here too, waiting times can stretch to several months, because the queues are long.
In Poland, therefore, it is not only possible, but extremely common, for a person experiencing symptoms of anxiety or depression whose condition is not severe to be admitted to psychiatric hospital to be left alone for weeks or even months.
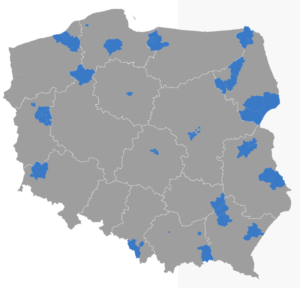
Those who live in a place where a community mental health centre has been opened as part of the national mental health care pilot programme are more fortunate. Here, each patient meets with a psychologist, before being referred to a doctor. In urgent cases, the appointment might be arranged within 72 hours. Yet there are just 29 such centres in Poland, and only people living locally are able to use them.
Sławomir Makowski – a clinical psychology specialist, psychotherapist, and chairman of the national board of the Polish Psychologists Union, outlines how this works in practice: “The assumption that people seeking help from centres in the new system will begin therapy fast is unfortunately incorrect – they have to wait as long as in clinics operating according to the old rules.” The new centres do not organise long-term psychotherapy or outpatient care, but rather refer patients to existing institutions.
“A positive change is meetings with a psychologist – after the initial contact we see a psychologist immediately,” continues Makowski. “To make an appointment to see a psychologist in the old system a patient first had to be referred by a psychiatrist, or the quicker option, which was a GP. That lengthens the time for obtaining psychological help.”
Excessive medicalisation
Apart from the difficulties with seeing a specialist and the social isolation of patients practised by larger hospitals, Polish psychiatry is also very medicalised.
Ksenia Sławińska, a specialist in clinical psychology and psychotherapist and head of the local branch of the Polish Psychologists Union at the Institute of Psychiatry and Neurology in Warsaw, explains why: “Because it’s cheaper than all other courses. It’s cheaper to give sedatives than to train staff how to help an agitated patient. Or to employ people who have these skills.”
To provide genuine help, pharmacotherapy should be combined with other interventions, especially psychotherapy. “Pharmacotherapy is necessary for controlling the symptoms of disorders – then you can start with psychotherapy,” explains Makowski. “But taking meds alone does not change the way of thinking, experiencing, functioning – so the source of the symptoms. Psychotherapy is therefore essential to make the change lasting, not only at the symptom level.”
Recovery is not easy
It is difficult to get better in this system. Mateusz Biernat managed it. “I began the recovery process when I met people who didn’t look at me through the diagnosis lens and helped me to regain my dignity and belief that I could live independently and achieve my own goals and decide for myself.”
This was very rewarding and a great trial of strength. According to a report on schizophrenia in Poland, the majority of people diagnosed with the condition do not work (74%). Only 19% have jobs, of which just 11% on a permanent contracted basis.
Why is this? Biernat blames the system: “People in a mental health crisis, who often have a history of profound trauma they deal with in various ways, often falling into addiction, end up where the system costs end up – in isolation. So as not to worry about them.”
After discharge from institutions, the state does not make it easy to return to independent life. “There’s a lack of initiatives to support these people so they can get an education or find work. At the moment, most people after leaving hospital enter a vacuum,” Biernat concludes bitterly.
“I’m currently a member of the mental health advisory board at the health ministry, and I also speak in the name of those whose voices are lost within the walls of the hospital or through social exclusion,” he adds. It is mostly NGOs and certain specialists who organise an annual mental health congress who are fighting for the rights of people with experience of mental health issues and living with diagnosed disorders.”
Important figures
One of the main reasons for the problems in the Polish mental health care system is, of course, funding. Poland is close to the rear of public health expenditure per capita in the EU, followed only by Bulgaria, Croatia, Romania and Latvia when figures are adjusted for price differences.
Total health expenditure in selected European countries (Euro per inhabitant, Eurostat)
*No data available for Poland in 2017
Poland spends just 3.7% – less than 3.5 billion zloty – of the entire amount available to its National Health Service on funding mental health care. The proportion in Germany is almost four times larger.
There is also a problem with the way mental health services are funded. Marek Balicki, a psychiatrist and former health minister and currently the head of the pilot schemes office of the national mental health programme, told OKO.press why it is in the interest of psychiatric hospitals to keep admitted patients in longer: “With inpatient care, the so-called person-day payment method applies. So no bed should be idle.”
Since a medical history has to be produced and various procedures carried out for each patient, it makes more sense to admit patients less often but for longer – because then there’s less work. Especially for already overworked staff on understaffed wards.
It is a different matter in mental health clinics, whose contracts with the National Health Fund (NFZ) depend on the number of consultations. “If they don’t do them, they won’t get money. So they register patients, fill in all the timesheets and only worry about everyone coming, because some patients make an appointment and don’t show up,” says Balicki.
Shortages of staff
Staff numbers are also a problem. There are nine psychiatrists per 100,000 Poles, whereas the figure in France is almost 23, and in Germany more than 27.
Number of psychiatrists per 100,000 inhabitants in 2016 (Eurostat)
The shortage of child psychiatrists is particularly serious. There are only around 400 in the entire country, meaning four per 100,000 residents. Furthermore, the distribution of specialists is uneven. Podlaskie province, for example, has no child psychiatry department. All such departments have overcrowded, often with extra beds in corridors, and it is not unusual to send young patients to other hospitals.
No one knows how many psychologists and psychotherapists there are. “Those data have never been available,” says Sławomir Makowski. “We’ve been appealing to the health minister for years to count the psychologists working in the public system. Estimates suggest a number around 40,000. Most work in training and pedagogical-psychological clinic – around 14,000 people – and in health care around 7-8,000.” Many of them work only part-time in public institutions, moonlighting in private practices.
One reason for the difficulty with access to these data is the lack of a functional law on the psychology profession. One was passed many years ago, but firstly it does not comply with EU regulations, and secondly, implementing provisions have not been made. “As a result, psychologists do not have a professional authority or register. And there’s no law at all on psychotherapists – it’s still being prepared,” says Makowski.
Pushed into the private system
An underfunded system pushes both patients and specialists into the private sector. The former because of long waiting times or a lack of suitable options. The latter, especially psychologists, because of low earnings. Not everybody can use the private system, for obvious reasons. Less affluent patients cannot afford a few hundred zloty per month for weekly sessions.
Makowski describes one of the absurdities of the Polish public system, which is driving specialists onto the private market: “Psychologists pay for a specialisation – even 800 zloty per month for four years. That’s around 40,000 zloty altogether (the price of a decent car), which they need to cover out of their own pocket.”
As well as specialisations, many psychologists invest in special courses to be able to conduct psychotherapy. These can cost even twice as much. “Increasing qualifications is such a large financial investment that in a hospital it would never be returned. This is why experienced psychologists and psychotherapists are leaving the state system for private practices, where they simply earn more,” Makowski concludes.
How much? Ksenia Sławińska does the sums: “Psychologists and psychotherapists don’t earn much – the average pay of a psychologist in health care is 3,000 zloty gross, 4,100 zloty for a specialist, so the respective net amounts are 2,000 (slightly more than the national minimum wage) and 3,000 zloty (much less than the average wage).”
As a result, experienced psychologists with a specialisation and certified therapists are lacking in the public system – and cannot be replaced by fresh graduates. Sławińska explains: “We’re missing the experience and skills of departing specialists. Therefore, psychologists beginning work in public institutions, even prestigious ones which are not short of applicants, have nobody to learn from.”
What is the NFZ doing about this problem? “A solution it introduced to deal with the specialist shortage was equalising the points for services performed by a certified psychotherapist with those performed by someone who has only completed two years of a psychotherapy course,” says Makowski.
“Its even worse with specialisations – the services of a clinical psychologist are evaluated similarly to those provided by people with two years’ clinical experience – meaning they have worked that many years in a hospital or clinic. Ridiculous,” he concludes.
During the pandemic
The coronavirus epidemic is an enormous challenge for an ossified system based on large institutions. Day care psychiatric wards, where patients come for psychotherapeutic sessions and psychiatric help, have been closed because of the epidemic, while inpatient psychiatric wards only admit people in cases of danger to life and health. Planned admissions, such as for diagnostic purposes, have been suspended.
Therapy is taking place by telephone. But psychotherapists have to come to work, as there is no system for working from home, involving secure medical documentation and connections. Some psychologists and therapists are unable to get to work, because they are looking after their children, for example. The result is that many patients have lost their psychological support.
Makowski points to another problem: “It would be hard to quickly set up a public crisis reaction system on an adequate scale with suitably qualified staff. Meanwhile, offers of psychological help have mushroomed, but it’s hard to verify who’s offering them. Theoretically, anybody could offer such support, and there’s no authority or register where you can check if that person is appropriately qualified.”
What about people in isolation? Mateusz Biernat warns: “Those with the misfortune to be in social exclusion, those experiencing isolation – at care homes or psychiatric hospitals – are the most exposed to the consequences of the epidemic. If a virus gets in from outside, it could have terrible consequences.”
The extent of the danger is shown by the example of Spain, where hundreds of residents of care homes died. In fact, a similar tragedy is already happening in Poland. The coronavirus has already attacked more than a dozen care homes and a psychiatric hospital in Warsaw.
What comes next?
Will the problems revealed by the epidemic lead to greater reform? We can only hope so – but the government has not announced plans to increase funding for mental health care. The impending economic crisis will leave the state with many other outgoings. People with mental disorders in Poland are stigmatised, and the thin slice – just 3.7% – of the small cake of health care funding hardly gives grounds for optimism.
Translated by Ben Koschalka
Main image credit: Tomasz Stanczak/Agencja Gazeta




















